
Page 16 - GALENIKA MEDICAL JOURNAL
P. 16
platform is prepared by placing three 10 mm trocars. The pressure of 14 mmHg column. Through three trocars, a
triangular groove of the GelPort platform has a connection camera with an optical instrument for image transmission
to the AirSeal device. The GelPort access channel is lubrica- onto a large screen and two working ports are inserted.
ted and inserted into the anal canal with the aid of an intro- During the procedure, we use standard laparoscopic 5 mm
ducer. The AirSeal insufflator is connected to the GelPort, graspers and ultrasonic scissors (ACE). At the beginning of
and its task is to provide a pneumorectum at a constant the operation, the rectal lesion is identified and marked
with an electrocautery hook along the perimeter, ensuring
clean, adequate margins in all directions.
Image 1. The GelPort platform is prepared for operation with the
AirSeal device connection set up We strive to achieve full-thickness resection of the wall
of the pathological lesion during surgical intervention,
allowing dissection down to the level of the mesorectal fat.
Upon completion of the resection, in a certain number of
cases, we perform a re-closure of the mucosal defect with
3-0 polyglactin (Vicryl) sutures without narrowing the lumen
of the rectum. The resected tissue specimen is extracted
through the GelPort membrane and sent for pathological
analysis.
Transanal excision in our institution was performed in
the standard manner with verification of the rectal lesion
and mapping of the rectum using conventional instru-
ments. After identifying the rectal lesion located 0 to 6 cm
from the anal verge, electroresection of the rectal lesions
was performed using either a conventional electrocautery
or LigaSure clamp with hemostasis control. All patients un-
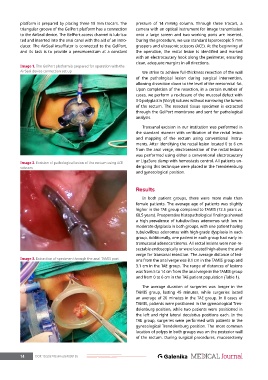
Image 2. Excision of pathological lesion of the rectum using ACE
scissors dergoing this technique were placed in the Trendelenburg
and gynecological position.
Results
In both patient groups, there were more male than
female patients. The average age of patients was slightly
higher in the TAE group compared to TAMIS (72.5 years vs.
68.5 years). Preoperative histopathological findings showed
a high prevalence of tubulovillous adenomas with low to
moderate dysplasia in both groups, with one patient having
tubulovillous adenomas with high-grade dysplasia in each
group. Additionally, one patient in each group had early in-
tramucosal adenocarcinoma. All rectal lesions were non-re-
sectable endoscopically or were located high above the anal
verge for transanal resection. The average distance of lesi-
Image 3. Extraction of specimen through the anal TAMIS port ons from the anal verge was 8.1 cm in the TAMIS group and
3.1 cm in the TAE group. The range of distances of lesions
was from 5 to 14 cm from the anal verge in the TAMIS group
and from 0 to 6 cm in the TAE patient population (Table 1).
The average duration of surgeries was longer in the
TAMIS group, lasting 45 minutes, while surgeries lasted
an average of 20 minutes in the TAE group. In 8 cases of
TAMIS, patients were positioned in the gynecological Tren-
delenburg position, while two patients were positioned in
the left and right lateral decubitus positions each. In the
TAE group, surgeries were performed with patients in the
gynecological Trendelenburg position. The most common
location of polyps in both groups was on the posterior wall
of the rectum. During surgical procedures, mucosectomy
14 DOI: 10.5937/Galmed2409015S